Supervised Autonomy
Supervised Autonomy
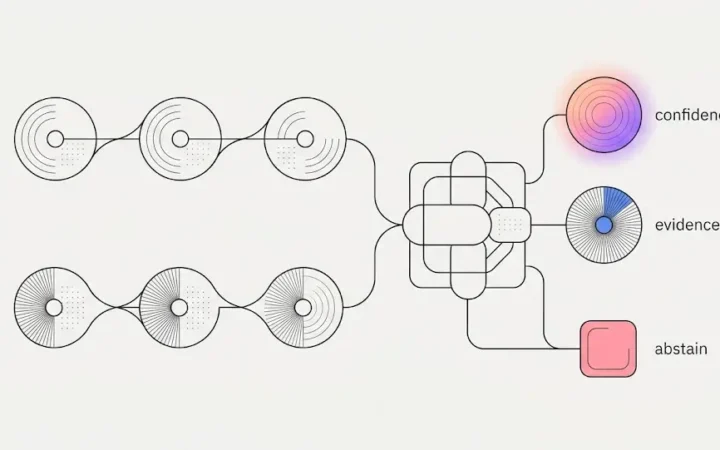
The Most Valuable Answer in Dental RCM Is “I Don’t Know”
Coverage determination isn't a model call — it's a data problem with two competing sources of truth and an obligation to be honest about uncertainty. Inside ELVA's RCM engine: derived payer-behavior rules, a judge that reviews every extracted rule, and a decision engine that abstains rather than guesses.
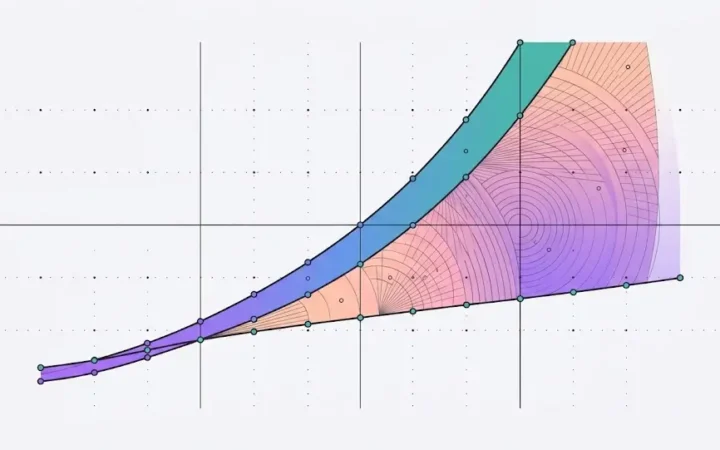
How to Grow Your Dental Group Without Growing the Overhead That Eats the Margin
Operational leverage — growing locations faster than the cost of running them — is the entire DSO investment thesis, and traditionally overhead eats it location by location. Here's how to grow a dental group without growing overhead in proportion, by removing the costs that scale with location count at the architectural level.
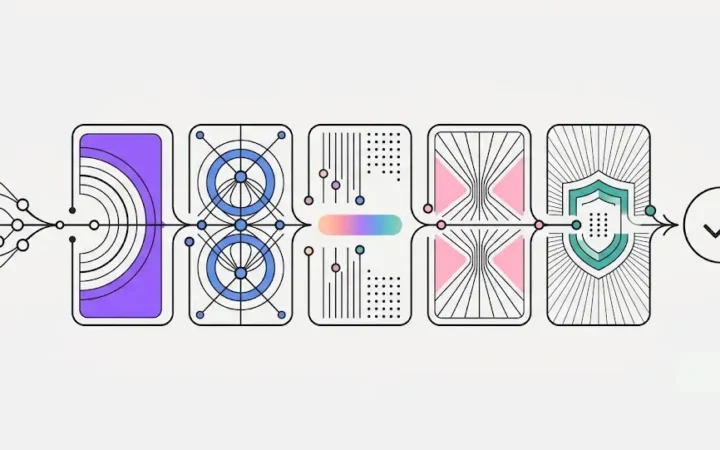
Can You Actually Defend Your AI to Your Board?
A solo practice adopts a tool because the owner likes it; a DSO has to defend it to a board, a sponsor, and a compliance function. Here's why "fully autonomous" AI fails that test — and the bounded, governed, auditable, scoped, and private posture that actually clears the bar.
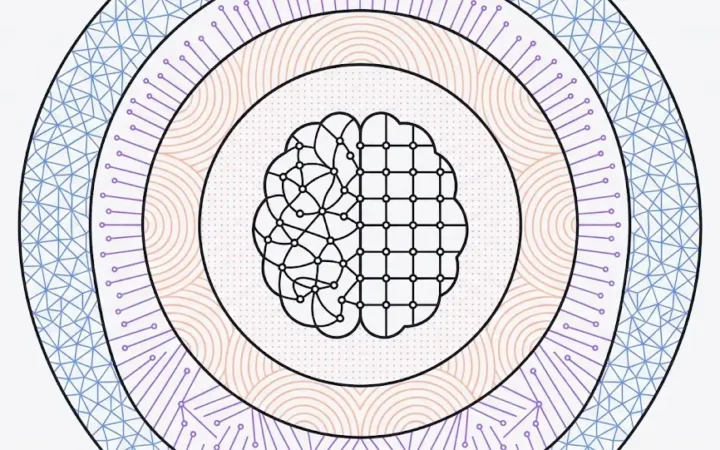
What “AI for Dentistry” Actually Requires: Inside the Architecture of a Practice Brain
Most "AI for dentistry" is a general-purpose chatbot with a dental prompt — fluent, ungrounded, and willing to guess. Here's what AI for dentistry actually requires at the architecture level: a neural-symbolic Practice Brain grounded in your real data and bound by your real rules.